Retake
M12) Chronic back pain and stiffness in a 32-year-old male
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with lower back pain.
- Review the DDx considerations in a patient with lower back pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with lower back pain.
History
A 32-year-old male visits his primary care physician's office, presenting with chronic back pain that began two years ago and has progressively worsened to involve his entire back. The pain and stiffness are most severe in the mornings but improve throughout the day. The patient experiences difficulty bending forward and turning his head, along with occasional hip pain. He describes the pain as a deep ache, with a severity of 6/10 at its worst, which is alleviated by NSAIDs. He denies experiencing fever, chills, or night sweats.
Physical Exam
Blood Pressure: 118/77 mmHg, Heart Rate: 66 bpm, Respiratory Rate: 18 breaths/min, Temperature: 37°C, O2 Saturation: 98%
Musculoskeletal: Mild tenderness on palpation of the sacroiliac joints and the entire length of the midline of the back. Limited range of motion in the right leg due to pain during abduction and flexion. Straight leg raise test is negative bilaterally.
Labs
HLA-B27: Positive
C-reactive protein (CRP): 37 mg/L (<10 mg/L)
Erythrocyte sedimentation rate (ESR): 75 mm/h (Reference range: 1-15 mm/h)
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient is most has ankylosing spondylitis. First, his symptoms, including chronic back pain, morning stiffness, and difficulty bending forward and turning his head, are classic features of this condition. Second, the patient's positive HLA-B27 test, elevated CRP, and ESR levels further support the diagnosis of ankylosing spondylitis as an inflammatory condition. Finally, the patient's age and the progressive nature of his pain also align with the typical presentation.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires routine workup and management as their condition is not immediately life-threatening.
First Imaging Study
What is the first imaging study you will order?
X-rays are the appropriate initial imaging study for detecting ankylosing spondylitis because they can reveal structural changes associated with the condition, such as sacroiliac joint involvement, syndesmophytes, erosions, “shiny corners”, vertebral body squaring, and ankylosis. Although X-rays have limitations, they serve as a valuable first-line imaging modality for evaluating patients with suspected axial spondyloarthritis, including ankylosing spondylitis.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
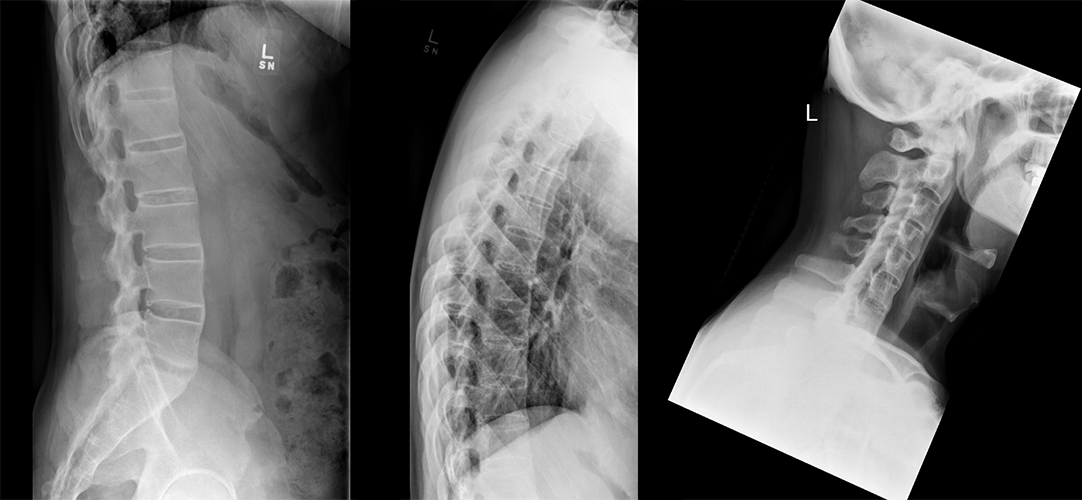
X-rays of cervical, thoracic, lumbar spine and hips
There is squaring of lumbar vertebral bodies:
Squaring of vertebral bodies is frequently observed in ankylosing spondylitis, often starting in the lumbar spine and affecting multiple levels.
There is ossification of supraspinous and interspinous ligaments:
The "dagger sign" appears as a single, central, radiodense line on frontal radiographs due to ossification of supraspinous and interspinous ligaments.
There is evidence of vertebral body fusion:
Ankylosing spondylitis can cause symmetric fusion of vertebral bodies by marginal syndesmophytes, creating a smooth, continuous "bamboo sign" appearance on x-rays.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
An MRI, while it has higher sensitivity and can detect earlier and more subtle changes in ankylosing spondylitis, is not necessary if the diagnosis has been confidently confirmed through an X-ray, particularly if there are no complications or atypical symptoms. MRI is generally used for diagnosis when the condition is suspected but not confirmed, for detecting early inflammatory changes before they appear on X-rays, or for evaluating treatment response or disease progression.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s presentation and imaging findings are consistent with ankylosing spondylitis.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires routine management as their condition is not immediately life-threatening.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 32-year-old male with a two-year history of chronic and progressive back pain, morning stiffness, and intermittent hip pain, showing relief with NSAIDs. Clinical exam, elevated inflammatory markers (ESR, CRP), positive HLA-B27, and imaging confirm the diagnosis of ankylosing spondylitis affecting the spine, SI joints, and hips. He should continue NSAID use for pain management and initiate physiotherapy for mobility. If symptoms persist or worsen, treatment with TNF-alpha inhibitors should be considered. Referral to an ophthalmologist for uveitis screening and rheumatology for further management and follow-up is recommended.
Lessons Learned:
- Individuals presenting with back pain due to ankylosing spondylitis typically report an insidious onset, improvement with exercise, no improvement with rest, pain at night (with improvement upon arising). Onset is usually <40 years old.
- Extra-articular manifestations of ankylosing spondylitis include acute anterior uveitis, inflammatory bowel disease, and psoriasis. Uveitis typically presents as acute unilateral pain, photophobia, and blurring of vision.
- Laboratory findings in ankylosing spondylitis are generally nonspecific. Elevated acute phase response biomarkers, including an elevated erythrocyte sedimentation rate (ESR) and elevated C-reactive protein (CRP) are often present in patients with active ankylosing spondylitis. Normochromic normocytic anemia may occur in patients with advanced disease.
- Radiographic findings of the SI joints range from subtle joint-space narrowing and sclerosis to erosive change and may eventually result in bony ankylosis (fusion). The three key radiographic findings of ankylosing spondylitis are the squaring of vertebral bodies, the dagger sign, and the bamboo spine sign.
Socioeconomic Factors: The occurrence of ankylosing spondylitis (AS) is closely linked to the presence of the HLA-B27 antigen, with variations among different ethnic groups, with the highest rates observed in those who are non-Hispanic white, followed by Mexican-American and non-Hispanic black. The condition predominantly affects males, according to multiple studies.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}